胰腺癌
胰腺癌(英语:pancreatic cancer)是指胰腺细胞发生癌变而产生的肿瘤,这些肿瘤细胞具有侵犯其他组织的能力[10]。胰腺的癌症可分为许多类型,最常见的是胰腺腺癌(pancreatic adenocarcinoma),占了85%,因此胰腺癌一词有时也用来直接指称胰腺腺癌,这些腺癌发源于胰腺制造消化酶的部位;该部位也可能发生其他几种通称为非腺癌(non-adenocarcinomas)的癌症。另外1-2%的病例为来自神经内分泌细胞的神经内分泌肿瘤,这类癌症的侵袭性通常没有胰腺腺癌强[6]。
| 胰腺癌 | |
|---|---|
 | |
| 胰腺位置示意图。此图的胰腺位于胃后方,图中橘色的为胃,黄色的为胰腺,紫色的为肝脏,绿色的为胆囊和胆管。 | |
| 症状 | 黄疸、腹痛、背痛、体重不明原因下降、浅色粪便、深色尿、食欲不振[1] |
| 起病年龄 | 40岁以上[2] |
| 风险因素 | 吸烟、肥胖症、糖尿病,罕见遗传因子[2] |
| 诊断方法 | 影像学、血液检查、组织切片[3][4] |
| 预防 | 戒烟、维持健康体重、减少食用红肉[5] |
| 治疗 | 手术、放射线疗法、化学疗法、和缓医疗[1] |
| 预后 | 五年存活率 5%[6][7] |
| 患病率 | 393,800(2015年)[8] |
| 死亡数 | 411,600(2015年)[9] |
| 分类和外部资源 | |
| 医学专科 | 肿瘤学 |
| ICD-11 | 2C10 |
| ICD-9-CM | 157.1、157.8、157.0、157.2 |
| OMIM | 260350 |
| DiseasesDB | 9510 |
| MedlinePlus | 000236 |
| eMedicine | 280605 |
| Orphanet | 1333、217074 |
胰腺癌最常见的症状和征象包括黄疸、腹痛或背痛、不明原因的体重减轻、浅色粪便、茶色尿和食欲不振[1]。疾病的早期通常没有症状,且这些症状通常不具特异性,因此发现胰腺癌时常常已经进展到癌症晚期[1][2],癌细胞已经远端转移到身体其他部位[6][11]。
胰腺癌很少发生在40岁以下的病人,半数以上的患者超过70岁[2]。胰腺癌的风险因子包括吸烟、肥胖、糖尿病和特定的罕见基因[2]。 约20%的胰腺癌和抽烟有关[3], 5–10%则和遗传因素有关[2]。胰腺癌的诊断常结合医学影像(超声波和电脑断层)、血液检验和组织切片等技术[3][4]。癌症分期则分为最早的第I期到最严重的第IV期[11]。目前尚无合适的方法能针对群众筛检胰腺癌[12]。
非吸烟者和少吃红肉或加工肉品的人罹患胰腺癌的风险较低[5]。吸烟者在戒烟后罹癌的几率会降低,戒烟20年后风险甚至能降到与一般人无异[6]。胰腺癌的治疗方法有手术、放疗、化疗、和缓医疗或结合上述数种疗法[1],疗法的选择和癌症的分期有关[1]。手术是唯一能治愈胰腺腺癌的方法[11],针对无法治愈的患者,手术则以提升生活品质为目标[1][11]。患者有时也会需要控制疼痛和促进消化的药物[11],即便是接受积极治疗的病人,也建议在疾病早期就实施缓和疗护[13][14]。
2015年,胰腺癌在全球已造成约411,600人死亡[9],为英国第五大死因[15],美国第四大死因[16][17]。胰腺癌于发达国家较常见,占了2012年新病例的70%[6]。胰腺腺癌的预后通常很差,一年存活率和五年存活率分别仅有25%和5%[6][7];早期诊断的五年存活率则提高到约20%[18]。神经内分泌肿瘤的预后则较好,诊断后的五年存活率约有65%,虽然患者预后仍需视个别癌症种类而定[6]。
种类
编辑
胰腺癌虽然有许多种,但可粗略归为两大类。绝大多数(约99%)的胰腺癌发生在胰腺的外分泌部(分泌消化酶的地方),此处的各种癌症在诊断和治疗上都有许多的共通点;另一些癌症则发生在胰腺的内分泌部(分泌激素的内分泌组织),特色和前者截然不同。这两类的胰腺癌都好发(但并非绝对)于40岁以上的患者,且男性稍多于女性,但少数亚型在女性和孩童身上较常见[19][20]。
外分泌肿瘤
编辑最常见的外分泌胰腺癌为胰腺腺癌(pancreatic adenocarcinoma)[注 1],占所有胰腺癌的约85%,约60%到70%的胰腺腺癌发生于胰头部[27]。
胰管是将胰腺外分泌腺的分泌物(例如酶以及碳酸氢盐)运输出胰腺的组织,尽管构成胰管的上皮细胞只占胰腺细胞总体积的10%[28],多数的胰腺腺癌始于胰管,称为胰腺管腺癌(pancreatic ductal adenocarcinoma,PDAC)[29]。
第二常见的胰腺癌为发源于胰腺外分泌腺体细胞的胰腺腺泡细胞癌,占胰腺外分泌癌症的5%,腺泡细胞会过度分泌特定的分子消化酶而导致如皮肤红疹和关节痛等症状[30]。
囊腺癌占了胰腺癌1%的病例,预后较其他外分泌胰腺癌佳[30]。胰母细胞瘤则是一种较少见的癌症,几乎都发生在孩童,且有相对较好的预后。其他胰腺癌的种类还包括腺鳞状细胞癌、印戒细胞癌、肝样细胞癌、胶状癌、未分化腺癌和具有蚀骨细胞样巨大细胞的未分化腺癌。固状伪乳头状肿瘤是一种罕见但低度恶性的肿瘤,主要发生在年轻女性,预后良好[2][31]。
胰黏液性囊性肿瘤包含多种胰腺肿瘤,且恶性程度不一。随着电脑断层技术的进步和普及,此类肿瘤的检出率也越来越高。此类肿瘤大多为良性,目前治疗及评估方法仍持续讨论中[32]。
神经内分泌肿瘤
编辑少数的胰腺癌由其他非外分泌的细胞造成,其中绝大部分为胰腺神经内分泌肿瘤(PanNET)[33]。神经内分泌肿瘤是一类多样的良性或恶性肿瘤,源自于协调神经与内分泌系统的神经分泌细胞。这类肿瘤能在体内多数的器官内产生(包括胰腺),但恶性的类别十分罕见。PanNETs可依其制造激素的能力分为“功能性”和“非功能性”两类,功能性肿瘤能将胰岛素、胃泌素或升糖素等激素分泌到血液中,过多的激素可能会产生对应的症状(例如过多的胰岛素造成低血糖),因此也较容易早期发现。多数的功能性PanNET为胰岛素瘤和胃泌素瘤,肿瘤依其分泌的激素种类命名。非功能性的PanNETs可能不分泌激素或分泌的量不足以造成明显的症状,因此此类肿瘤常在扩散到身体其他地方后才被诊断出来[34]。
如同其他部位的神经内分泌肿瘤,PanNETs的分类和命名历史相当复杂[33],它有时又被称为胰岛癌[35],虽然目前已知这些癌细胞并非都源自胰岛细胞[34]。
症状及征象
编辑
胰腺癌初期通常没有明显的症状,因此通常都是在转移后才发现[4],这也是胰腺癌一般预后极差的原因之一。但胰腺神经内分泌细胞瘤(PanNETs)除外,此类肿瘤可能会分泌过多的激素而造成对应的症状(症状类型需视其分泌的激素种类而定)[36]。
胰腺癌多半发生在40岁以上的人,在胰腺腺癌被诊断出来之前常会发生以下症状:
- 上腹痛或背痛:通常发生在胃的周围以及此处往背部延伸的部位。疼痛的位置和肿瘤的位置相关,患者可能晚上睡觉时较痛,疼痛随时间增加而不会缓解[30],将身体前倾能稍微纾解症状。英国有一半的胰腺癌病例是患者因疼痛和黄疸前往急诊室而被诊断出来的,其中多达2/3的患者以腹痛为主诉,46%的患者伴随黄疸,而13%的患者有黄疸但无腹痛[11]。
- 疼痛或无痛性的黄疸(皮肤或眼白变黄):当肿瘤位于胰腺的头部而造成总胆管阻塞时便会发生,有时也可能伴随黑尿[37]。
- 不明原因的体重减轻:这可能是食欲不佳或外分泌腺体失能而导致消化不良的结果。[11]
- 消化道症状:肿瘤也可能压迫周围的器官,阻碍消化道并造成胃排空困难,进而引发恶心、呕吐、饱足感等症状。未消化的脂肪会导致恶臭且冲水冲不掉的脂肪泻[11],便秘也是常见的临床表现[38]。
- 糖尿病:至少一半的胰腺腺癌患者在被诊断出来的当下患有糖尿病[2]。虽然已知长期糖尿病是胰腺癌的风险因子,但胰腺癌本身也可能造成糖尿病,因此近期才发作的糖尿病也有可能是癌症的早期表现[39]。50岁以上的糖尿病患者三年内罹患胰腺腺癌的几率是常人的8倍,但三年后患上癌症的几率则逐渐降低[11]。
其他表征
编辑- 游走性血栓静脉炎:门脉、四肢深层静脉或身体各处表浅静脉的血栓生成可能也和胰腺癌有关,10%的患者有此现象[3]。
- 重性抑郁障碍:10–20%的胰腺癌患者会变得忧郁并排斥治疗,此现象也可能在诊断出癌症前就发生,代表忧郁可能是癌症本身透过生理机制造成的[3]。
其他常见的表征还包括:虚弱、疲劳、口干、睡眠问题、可触摸的腹部肿块等[38]。
远端转移后的症状
编辑
胰腺癌的远端转移也可能造成症状。典型的胰腺腺癌会先散播到邻近的淋巴结,接着再扩散到肝脏、腹膜腔、大肠或肺脏等处[3],转移到骨头或大脑的状况则不常见[40]。
胰腺内的肿瘤也可能来自身体的其他地方,但这种状况很少见,仅占所有胰腺肿瘤的2%,其中又以肾脏癌最多,其次是大肠癌、黑色素瘤、乳癌和肺癌。一般可以用手术来移除这些肿瘤以治疗或减轻症状[41]。
风险因子
编辑- 年龄、性别、族裔:罹患胰腺癌的风险随着年龄增加,多数的患者超过65岁,小于40的患者较少见。胰腺癌在男性的发生率略高于女性。美国的统计指出非裔美国人的发生率较平均高出1.5倍,但胰腺癌在非洲的发生率并不高[6]。
- 吸烟:为目前研究最为透彻且可以避免的胰腺癌风险因子,长期吸烟罹患胰腺癌的风险大约会增为2倍,且风险随烟龄增加。戒烟后风险会缓慢下降,大约20年后才能回复到与非吸烟者无异[43]。
- 肥胖:BMI 大于35的人风险约为一般人的1.5倍[11]。
遗传性
编辑5–10%的胰腺癌患者家族成员也有该病病史[2][44]。若多于一位一等亲罹患该疾病,患病几率会大幅增加,且常在50岁之前发病[4]。遗传性胰腺癌会提升70岁以前的发病风险约30–40%[3]。大多数与胰腺癌相关的基因目前仍属未知[2][45]。针对高遗传风险的患者,可以进行早期筛检,但由于目前已知的因子不足,筛检无法完全防范[46]。有些人甚至会选择预防性切除胰腺[3]。
- 珀茨-杰格斯综合征:与STK11肿瘤抑制基因相关。此疾病相当罕见,但为强风险因子。
- 发育不良母斑综合征:又称家族性非典型多痣黑素瘤(familial atypical multiple mole and melanoma syndrome,FAMMM-PC),与CDKN2A抑癌基因相关。
- 共济失调微血管扩张综合征:与体染色体隐性的ATM基因,以及体染色体显性的BRCA2和PALB2基因相关。
- 遗传性非瘜肉症结直肠癌
- 家族性结直肠瘜肉综合征
- 多发性内分泌肿瘤第一型(MEN1)及希佩尔-林道综合征:与胰腺神经内分泌肿瘤相关。
酒精
编辑酗酒是造成慢性胰腺炎的主要原因,慢性胰腺炎患者也比较容易罹患胰腺癌。然而,诸多研究却都无法证实酒精饮用量是罹患胰腺癌的直接风险因子。整体而言,这两者的关联性很低,多数的研究甚至得到两者没有关联的结论,但在统计分析中,吸烟是个很强的干扰因子。大量饮酒则和胰腺癌有比较强的关联[47][48]。
高血糖
编辑糖尿病是胰腺癌相当重要的风险因子,新发病的糖尿病患者也可能会有上述的各种征象。被诊断为2型糖尿病达10年以上的患者比非糖尿病患者多出了50%的风险[49]。高血糖会导致核糖核苷酸还原酶(RNR)被糖基化,导致其活性减低,造成胰细胞合成核苷酸的能力降低,干扰细胞内的DNA修补系统,进而提高KRAS基因突变的机会[50]。
其他
编辑诊断
编辑

胰腺腺癌在初期不会有任何特殊症状,目前也没有较好的鉴别诊断方式[11][3][37],其症状随肿瘤的位置不同而异。
不论肿瘤具体位置,胰腺癌最常见的症状为不明原因的体重减轻。35-47%的人有恶心、呕吐和虚弱感。胰头的肿瘤还可能导致黄疸、疼痛、食欲不振、茶色尿及浅色粪色。胰体及胰尾的肿瘤则可能导致疼痛[37]。
胰腺癌发病时,患者可能同时伴有最近发生且难以控制的非典型2型糖尿病,或病因不明的血栓静脉炎(即特罗索氏征),患者也可能有胰腺炎病史[37]。超过五十岁的糖尿病患者伴有不明原因的体重减轻、持续腹痛或背痛、消化不良、呕吐以及脂肪便等典型症状时,医师便会怀疑患者有胰腺癌[11]。黄疸伴随无痛的胆囊肿胀(即库尔瓦泽尔兹氏征)也进一步增加了胰腺癌的可能,并能帮助胰腺癌与胆结石的鉴别诊断[54]。
胰腺癌可借助电脑断层(CT)或内窥镜超声波(EUS)等医学影像技术确诊,并协助判断肿瘤是否能以外科手术切除[11]。在配合显影剂使用的计算机断层成像中,胰腺癌会慢慢的吸收显影剂,而正常的胰腺组织则会将显影剂快速排除,慢性胰腺炎排除显影剂的速度则较慢[55]。核磁共振和正子计算机断层成像也可用来诊断胰腺癌[2];在某些案例中,核磁共振胆胰管摄影术也很有用[37]。 腹部超声波的敏感度较低,可能会遗漏较小的肿瘤,但能协助诊断散播到肝脏或腹水中的肿瘤[11];由于腹部超声波便宜又快速,在做其他检查前也能以此做初步的检查[56]。
若诊断尚有不明之处,则可以内窥镜超声波术辅助细针抽取细胞检查做病理诊断;但对于势必要切除肿瘤的病患则不一定需进行细针病理切片[11]。
肝功能测试为胆道郁积的指标(包括共轭胆红素、γ-GT、碱性磷酸酶增加)。CA19-9为胰腺癌患者体内常提升的一种肿瘤标记;但有5%的人缺乏路易士抗原系统,因此无法制造该蛋白。CA19-9诊断胰腺腺癌的灵敏度约80%,特异度约73%,灵敏度和特异度皆不够高;比起用于诊断,该标记更适合用来追踪已确诊病人的病况[2][11]。
最常见的胰腺癌为胰腺腺癌,显微镜镜检下以中度到低度分化的腺体结构为特色,通常伴有大量的结缔组织增生,也可能有致密纤维基质(如第一型胶原蛋白和透明质酸沉积)与细胞(包括肌纤维母细胞、巨噬细胞、淋巴细胞、肥大细胞)产生。这些组织变化创造了缺乏血管和氧气的肿瘤微环境[2],造成许多化疗药物无法到达肿瘤所在,使得此类癌症难以治疗[2][3]。
分期
编辑外分泌肿瘤
编辑胰腺癌的分期通常必须借助电脑断层[37],最常使用的分期系统是美国癌症联合委员会(AJCC)与国际抗癌联盟(UICC)共同制定的系统。AJCC-UICC分期系统将胰腺癌根据TNM系统分为四期,“T”代表肿瘤的大小,“N”代表淋巴结扩散程度,“M”则代表远端转移[57]。
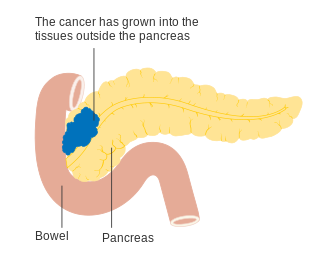
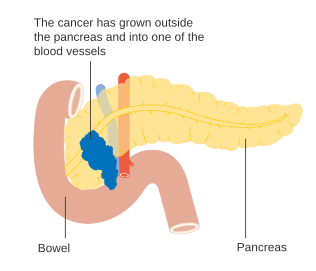
为了辅助判断后续治疗,肿瘤也可根据是否可以手术切除来分为“可切除”(resectable)、“临界可切除”(borderline resectable),以及“无法切除”(unresectable)等三大类[58]。如果肿瘤仍为初期(AJCC-UICC第一期或第二期),尚未扩散到血管或远端器官,则建议最好进行手术切除[11]。AJCC-UICC分期系统的第三期包括了“临界可切除”(borderline resectable,指腹腔动脉和上肠系膜动脉仍未被波及而能动手术者)和“不可切除”(局部侵犯更严重的)的胰腺癌;对应到详细的TNM分级的话,这两者分别为T3和T4[3]。
- 胰腺癌分期(TMN分期系统)
-
 胰腺癌T1期
胰腺癌T1期 -
 胰腺癌T2期
胰腺癌T2期 -
 胰腺癌T3期
胰腺癌T3期 -
 胰腺癌T4期
胰腺癌T4期 -
 邻近淋巴结的胰腺癌,N1期
邻近淋巴结的胰腺癌,N1期




_CRUK_178.svg)
_CRUK_179.svg)
局部侵犯较严重的肿瘤可能会波及以下邻近器官(粗略按照发生率递减排序):十二指肠、胃、横结肠、脾脏、肾上腺和肾。肿瘤也很常散播到胰腺周围重要的血管、淋巴管或神经,让手术变得困难许多。第四期癌症典型的远端转移位置有肝脏、腹膜腔和肺,50%以上的转移位置都在这三个器官[59]。
神经内分泌肿瘤
编辑2010年WHO消化系统肿瘤分类将所有胰腺神经内分泌肿瘤(PanNETs)依据其细胞分化程度分为三级,包括从分化程度最好的NET G1到分化很差的NET G3[20]。美国国家综合癌症网络则建议对神经内分泌肿瘤采用和胰腺腺癌相同的AJCC-UICC分期系统[60]:52,然而在这个系统下,PanNETs和相同分期的外分泌肿瘤预后并不相同[61]。此外,欧洲神经内分泌肿瘤协会另有提出一种不同的TNM分类系统[20]。
癌前病变
编辑_Case_01.jpg)
外分泌肿瘤
编辑
此类肿瘤一般认为源自于数种胰内的癌前病变,但这些病灶未必一定会演变为癌症。随着电脑断层的普及及进步,有越来越多的上述病灶被侦测出来,此类病灶未必需要治疗[3],这些病灶中最常见的为胰浆液性囊腺瘤,此类几乎都为良性,除此之外还有另外三种病理状态:
第一种为胰腺上皮瘤病变,属于组织病变。这类病变通常发现于生前无癌症报告的法医学诊断。此类病灶拥有分级系统,恶性度最高者即为恶性肿瘤。90%以上病例拥有KRAS基因突变,2至3级则可能额外还有CDKN2A (p16)、p53 、SMAD4等基因的突变[2]。
第二种为胰管内乳头状黏液性肿瘤(IPMN),成人盛行率约2%,到70岁时则提升到约10%,而其中25%有成为恶性肿瘤的风险。这些肿瘤常有KRAS基因突变(40-65%)和影响Wnt讯息传递路径的GNAS与RNF43突变[2]。即使在手术切除肿瘤后,患者之后罹患胰腺癌的几率仍然比常人高出许多[3]。
最后一种则是主要发生在女性的胰黏液性囊状肿瘤(MCNs),它可能维持良性或发展为恶性[62]。如果肿瘤变大、造成异常症状或有任何可疑的特征,医师通常能借由手术将肿瘤完整切除[3]。
胰管腺癌的基因变化已经被详细研究,较常见的癌症类型也已经有完整的外显子体定序。胰腺腺癌有四种主要的基因突变:KRAS(95%)、CDKN2A(95%)、TP53(75%)和SMAD4(55%),其中拥有SMAD4突变的肿瘤预后较差[3]。SWI/SNF突变或缺失也出现在10–15%的胰腺腺癌案例中[2]。其他一些类型的胰腺癌和胰腺癌前病变的基因变化也已有研究发表[3]。
神经内分泌肿瘤
编辑胰腺神经内分泌肿瘤(PanNETs)常见的突变基因和胰腺腺癌不同[63]。例如PanNETs通常没有KRAS突变,但却常有遗传性的MEN1基因突变,造成MEN1综合征(一种常造成多种原发性内分泌肿瘤的遗传性疾病),带有MEN1突变基因的人大约40-70%会罹患PanNet[64]。其他常见的基因突变包括DAXX、mTOR和ATRX[34]。
预防和筛检
编辑除了不要抽烟之外,美国癌症协会也建议人们维持健康的体重、增加蔬果和全谷的摄取,同时减少食用加工肉品,虽然目前没有明确的证据显示这能有效预防并降低罹患胰腺癌的几率[65]。一份2014年文献回顾总结了先前的研究,指出增加柑橘和姜黄的摄取能减少胰腺癌的风险,而全谷、叶酸、硒和非油炸的鱼肉可能也有帮助[66]。
目前仍没有适合对群众筛检的方法,新的技术和针对特定族群的筛检方法还正在研究评估[67][68]。然而,对高遗传风险的族群而言,使用内窥镜超声波和MRI/CT造影是目前建议的例行性筛检方式[4][56][68][69]。
处置
编辑外分泌肿瘤
编辑肿瘤是否能以手术切除是胰腺癌确诊后重要的评估项目,因为手术切除是目前唯一治愈该病的方法。而肿瘤能否切除则取决于它侵犯和扩散的程度,肿瘤本身的位置也是个重要的因子,CT能显示出病灶与胰腺附近血管的相对位置。病患自身的健康状况也需被评估,虽然年龄本身并不是手术能否进行的决定性因素[3]。
无论是否能进行手术,多数的患者会接受化疗和放疗(后者较少)。胰腺癌的处置需要跨领域团队合作进行,包括肿瘤科等专家,因此在大型医学中心处置会是最好的选择[2][3]。
手术
编辑
大约只有20%的胰腺癌有手术治愈的机会[11],虽然CT很有帮助,但要判断肿瘤是否能完整移除仍然十分困难,很可能手术进行时才发现肿瘤无法在不破坏其他维生器官的情形下完整移除。决定是否进行手术受到许多因素影响,包括肿瘤确切的解剖位置是否靠近或侵犯到静脉或动脉[2] 、外科技术以及术后复原的考量等[70][71]。患者的年纪本身并非决定手术与否的条件,但其综合日常体能状态必须足以支应大手术带来的冲击[11]。
肿瘤和周围的血管之间是否有明显的脂肪作为分界是手术评估的一项重要指标,若肿瘤与血管有明显区隔者较适合进行手术[3],传统上会测量肿瘤到邻近主要动脉或静脉的最短距离,并以相邻(abutment,指肿瘤与血管的距离不足该血管圆周的一半且无脂肪分隔两者)、包围(encasement,指肿瘤包围大部分的血管壁)或全血管侵犯(full vessel involvement)来描述肿瘤与血管之间的关联[72]:22。包围血管的肿瘤在一些情形下是可行的[73][74],特别是能使用前导性化学治疗[75][76][77]、化疗[71][72]:36[78]或放疗[72]:29–30的时候。
即使手术表面看来成功,肿瘤边缘剩下组织的病理切片却常会发现癌症细胞,这意味着癌症细胞并未完全被移除[2];更糟的是,癌干细胞在显微镜下并不是很明显,它们可能继续发展为癌细胞并往外扩散[79][80]。因此,术后可用腹腔镜检查(一种小型、影像导引的手术)更进一步地了解手术后的整体成效[81]。

针对涉及胰头的癌症,最常使用的手术方法是胰十二指肠切除术,这是个将胰头连同十二指肠一起切除的大手术,术中切除十二指肠后会将胃和空肠相接,并留一段空肠的盲端来导引胆汁。这项手术只有在病人身体足以承担大型手术,且癌症并未局部扩散或转移时才会采用,因此只有很少数的病例进行胰十二指肠切除术。 胰尾的肿瘤则能用远端胰切除术移除,手术中也常会将脾脏一并切除[2][3]。现在这些术式常能以微创手术完成[2][3]。
虽然在1980年代以后,以治愈为目标的手术不再意味着高死亡率,但仍有许多患者(约30至45%)必须接受术后治疗,以处理非癌症本身导致的术后并发症,其中最常见的并发症为胃排空障碍[3]。一些较局部的手术也能用来减轻症状,但就不是以治愈癌症为目标,例如在侵犯十二指肠或大肠的案例中便能借由绕道手术来维持患者消化道的畅通,藉以增进患者的生活品质,但无法根治癌症[11]。
化疗
编辑若病人的情况许可,可在手术后一段时间给予吉西他滨或5-FU等药物进行辅助性化疗,通常辅助性化疗会在术后一至两个月实施[4][56]。对于身体情况不允许进行治愈性手术的病患,化疗或许可以延长其生命或提升生活品质[3]。临界可切除(参见分期一节)的病患,可在术前进行前导性化疗或化放疗可能可以使肿瘤缩小至可以切除的程度。除上述情形以外,进行前导性化疗与否仍有争议,但可以延迟手术的进行[3][4][82]。
吉西他滨在临床试验证明可以改善生活品质,并可延长存活中位年数长达五周后,于1997年获美国食品药品监督管理局(FDA)核可使用于胰腺癌[83]。在本品的临床试验之前,药物的效果基本上仅以存活率评估。吉西他滨是FDA首支以临床效益(clinical benefit)核可的药物[84]。此后长达十年的时间胰腺癌化疗的标准疗程都只单用吉西他滨,其他药物组合试验都没有更显著的效果。直到后来吉西他滨与厄洛替尼可以稍微提升存活率,厄洛替尼也于2005年核准用于胰腺癌的化疗[85]。
FOLFIRINOX化疗处方利用了四种药物,比单独使用吉西他滨更有效,但具有严重的副作用,因此仅适用于体能状态较佳者。副作用同样较强较强的还有蛋白结合性紫杉醇(nab-paclitaxel),该药与吉西他滨并用治疗胰腺癌的疗法于2013获FDA核可[86]。截至2013年底,对于体能状况较佳者,上述两种疗法是较佳的选择。而对于体能状况不许可者,则可单独使用吉西他滨。两种疗法的平行对照研究仍在进行当中,并有许多其他疗法的研究也在持续进行中。但前几年的研究都仅能较原疗法延长数个月寿命[83]。有多项临床试验研究经典辅助性疗法的效果[4]。
放射线疗法
编辑手术后进行辅助性放疗的效果至今仍未有共识[3]。欧洲肿瘤学学会建议仅对注册进行临床试验者进行放疗[56],美国则相较欧洲来说对放疗持更积极的态度。自1980年代起,学界便进行许多临床试验,但迄今仍未获得明确结果[3][4]。
放疗也许又助于将肿瘤缩小至可切除的大小。但对于不可切除的肿瘤而言,研究的结果仍有歧异。2013年一项研究的初步结果显示放疗可降低局部晚期肿瘤的活跃程度[2]。
神经内分泌肿瘤
编辑胰腺神经内分泌肿瘤(PanNETs)的有多种治疗方式,此类的恶性肿瘤较为罕见[60][87][88][89]。一些偶然发现的小型肿瘤(小于1公分),例如因为其他目的而做计算机断层成像时发现者,可能会先采取观察性等待的消极策略[60]。采用何种策略取决于手术的风险评估以及患者产生其他共病的几率[60],例如局限于胰腺内或仅小范围转移的肿瘤可能就会以手术切除,手术的方式则端看肿瘤的位置和淋巴结扩散的程度[20]。
相较于胰腺腺癌,局部的神经内分泌肿瘤切除手术需要切除的范围小很多,除此之外手术的方式皆与外分泌肿瘤相同。术后的预后差异很大,有些类型的存活率很高,有些死亡率则较高。由于无论是哪种类型的神经内分泌肿瘤都很少见,医疗指引强调这类病患需在专门的医学中心诊治[20][34]。若肿瘤有肝脏转移,肝脏移植也是可以考虑的选项[90]。
功能性肿瘤(即会分泌激素的肿瘤)可以使用体抑素类似物等药物(如奥曲肽)来减少激素的产生[20],兰瑞肽(lanreotide)则能减缓肿瘤的生长[91] 。如果肿瘤不适合以手术移除但却造成不适的症状,以癌伏妥或舒尼替尼等药物进行标靶治疗或许能减缓症状和病程[34][92][93]。标准的胞毒性化疗一般而言对PanNETs没有用,但当其他药物治疗失败时也可用来试着减缓病程[34][94],有时也用在分化不佳的PanNETs[95]。
若肿瘤持续向外扩张(例如转移到骨头),有时也会考虑使用放射疗法。此外,一些PanNETs会吸收特定的多肽或激素, 因此能采用核子医学疗法,以带放射性的多肽或激素治疗(例如碘苄胍,即碘-131-MIBG)[96][97][98][99]。射频烧灼术(RFA)、冷冻消融术和肝动脉栓塞也是可以考虑的治疗方式[100][101]。
安宁疗护
编辑安宁疗护着重于疾病的症状治疗,目的在减轻病患的痛楚、增进患者生活品质[102] 。由于胰腺腺癌常到后期才被诊断出来而难以治愈,在这种情况下,安宁疗护成了唯一可行的治疗方式[103]。安宁疗护并不以根治疾病的源头为目标,而是要缓解如疼痛或恶心等症状,并协助患者对决定往后的疗程与规划,包括是否住进安宁病房等重大医疗决策[104],疼痛的常见处置方式则有使用鸦片类药物或进行手术。
腔神经丛阻断术(CPB)截断了负责传递腹部疼痛的神经,因此能舒缓腹部疼痛的感觉,这是一种安全且有效的方式,患者在术后能减少鸦片类药物的使用量,进而避免药物相关的副作用[3][105]。另一种能借由手术缓解的症状为肿瘤导致的肠道或胆管阻塞,超过一半的胆管阻塞患者能以内窥镜手术置入金属支架,维持胆管的畅通[37]。安宁疗护也帮助解决被诊断出癌症后伴随而来的忧郁症[3]。
胰切除术或无法手术的大肿瘤常因为胰腺的外分泌功能不足而导致消化系统问题,这样的症状可以服用人工生产的胰脂肪酶来解决,此类酵素配饭吃效果最好[11]。胃排空障碍也是很常见的问题,症状有时会严重到必须住院,胃排空障碍的治疗方式有很多,包括鼻胃管引流、服用氢离子泵阻断剂或组氨酸H2受体拮抗剂,后两种药物能够减少胃酸分泌[11]。甲氧氯普胺等促进消化道运动的药物也能用于协助胃排空[106]。
预后
编辑| 临床分期 | 五年存活率(%):美国,1992–98年 | |
|---|---|---|
| 外分泌性胰腺癌 | 接受手术后的神经内分泌肿瘤 | |
| IA / I | 14 | 61 |
| IB | 12 | |
| IIA / II | 7 | 52 |
| IIB | 5 | |
| III | 3 | 41 |
| IV | 1 | 16 |
由于胰腺腺癌和其他较少见的外分泌肿瘤多半都到末期才被发现,肿瘤已经严重的侵犯周围组织或转移,因此预后通常很差[2]。胰腺神经内分泌肿瘤的预后则乐观许多,其中有很多个案是良性且没有任何临床症状的,即使是无法以手术治疗的患者五年存活率平均也有16%[58],其预后很大部分取决于神经内分泌肿瘤的类型[36]。
局部侵犯较严重或已转移的胰腺腺癌占了超过80%的病例,针对这些患者,许多比较化疗配方的临床试验显示这些药物能延长存活时间,但不超过一年[2][83]。美国的胰腺癌五年存活率已经从1975到1977年的2%进步到2003到2009年间的6%[107]。仅有20%的患者在胰腺腺癌还很小且局限于病灶处时被诊断出来(小于2公分,处于T1期),针对这些患者,美国的五年存活率为20%[18]。
流行病学
编辑
截至2012年,胰腺癌在全球已造成约330,000人死亡[6]。比2010年多出了20,000人[108]。光是在2016年的美国,就有53,070人新检出胰腺癌,41,780人因此而死亡。虽然胰腺癌只占新检出病例的3.1%,但却占了该年死亡率的7%[109]。
胰腺癌为造成全球癌症死亡人数第七高的疾病[6]。在女性为常见癌症的第11名,男性则为第12名[6]。多数案例发生于发达国家[6]。美国人胰腺癌的平均累积发病率约为每67人中一位(约1.5%) [110],较英国稍高[111]。其中男性病患较女性为多[6][2],但近年内,两性之间的差异在逐渐缩小,可能与过去女性抽烟率的上升有关。在族裔部分,非裔美国人的发生率较白人高出了50%,但非洲与东亚的发生率则远低于北美及欧洲。美国、中欧、东欧、阿根廷,及乌拉圭的发生率较高[6]。
胰腺癌为英国第十大死因(2011年约有8,800名新病例),并为致死人数第五高的癌症(2012年约有8,700死亡)[112]。
神经内分泌肿瘤
编辑根据临床诊断,胰腺神经内分泌肿瘤(PanNETs)的年发生率并不高(每年每百万人中约5人),且大多数为非功能性型[31],约占PanNET的45%至90%[20][34]。然而遗体解剖则发现小型的PanNETs比例其实相当高,代表有高比例的肿瘤是无症状的[34]。PanNET约占所有胰腺癌的1-2%[31]。此类疾病的定义时常变动,使其流行病学和临床相关性的知识常常受到影响[63]。
历史
编辑1761年,有“现代解剖病理学之父”之称的意大利科学家乔瓦尼·莫尔加尼,在其论文〈五具遗体的病理解剖报告〉('De Sedibus Et Causis Morborum Per Anatomen Indagatis Libri Quinque.')中首次提及胰腺癌[113]。但由于缺乏显微镜的证据,无从判断这份报告的结论是否正确。且由于胰腺癌在巨观下与胰腺炎相当类似,当时许多医师质疑原发于胰腺的癌症是否存在[114]。直到1858年,美国的雅各布·曼德斯·达·哥斯达医师发表了首篇附上显微镜检结果的胰腺腺癌诊断,才正式证实了胰腺腺癌的存在[113]。至20世纪初,发生于胰腺头的癌症已经有相对成熟的诊断方法[114]。
胰腺的神经内分泌肿瘤(PanNETs)则直到1888年才首次提及,首例因PanNETs造成的胰岛素过高病例报告于1927年发表。1955年,美国外科医师R·M·索林格(R. M. Zollinger)和E·H·艾利森(E. H. Ellison)于两例异常严重胃溃疡的病例报告中,推测胰腺分泌胃泌素细胞发生肿瘤的可能性,此后这种疾病也依两人的名字命名为索林格-艾利森氏综合征,一般文献认为这是首次发现非胰岛素性的PanNETs[114]。2010年,世界卫生组织建议将PanNETs从“内分泌肿瘤”归入“神经内分泌肿瘤”之列[33]。
1898年,意大利外科医师亚历山德罗·科迪维利亚执行首例胰十二指肠切除术,但后来患者在18天后即因并发症去世。早期医师误以为十二指肠为人类存活之必须,因此完全不考虑切除。同时胰液的引流也是当时争论不休的话题,一开始有人认为胰液的流向是生存的关键,但随即有人发现胰液于何处进入肠道与存活无关。然而,这却造成某些医师误以为将胰管完全结扎不会有任何副作用,但事实上这么做会导致瘘管的产生,使胰液渗入腹腔。1907–08年间,在经过多例不成功的手数后,法国外科医师开始在尸体上进行模拟手术,研究手术流程[115]。
1912年,德国外科医师瓦尔特·考施于波兰弗罗茨瓦夫的布雷斯劳,进行首次同时移除胰腺及大部分十二指肠的手术。1918年,有人证实将狗的十二指肠切除,犬只仍能继续存活,但直到1935年,美国医师艾伦·惠普才首次在人类身上切除十二指肠。当时惠普于纽约市的哥伦比亚长老教会医院进行三例手术,其中一名分两阶段完全切除十二指肠,并且存活了两年后才死于肝转移。这次手术完全是出自偶然,因为肿瘤是在手术室内才发现。惠普的成功为胰腺癌手术的发展奠定了重要的基础,但时到今日,胰十二指肠切除术仍是相当具有挑战性,且风险极高的手术。惠普并于1940年进行首例一阶段性十二指肠全切除术,此后也持续改良其术式,一生共进行了37次胰十二指肠切除术[115]。
1930年代末期发现维生素K能预防出血,同时输血技术也大幅进步与普及,使得术后存活率大幅增加[115],但直到1970年代以前,25%的患者在术后始终无法活着离开医院[116]。1970年代,一个美国的外科团队甚至力劝医界废除此种手术,因为它实在是太过危险。但也是从同时期开始,大型医学中心胰腺癌手术的预后大幅好转,手术死亡率逐渐降到4%以下[117]。一份2006的研究发表了约翰·霍普金斯医院一位外科医师的手术报告,该医师在1969和2003年间执行了1000例胰十二指肠切除术,其中1980年以前只有3例,在此段期间内的手术存活率稳定上升,手术时间的中位数也从1970年代的8.8小时缩短到2000年代的5.5小时,30天内或住院期间的死亡率则仅有1%[115][116]。另一系列由麻省总医院在1941和2011年间执行的2050例手术也呈现类似的变化趋势[118]。
利用现代医学影像技术,发现胰腺肿瘤癌前病变的比例逐渐提高,例如日本研究者在1982年首次发表了胰管内乳头状黏液性肿瘤(IPMN)。2010年的一份文献称“未来十年可能不会有人注意到这份文献,但接下来的15年,对胰腺癌的认识会有爆炸性的成长。”[59]
研究方向
编辑目前世界各国对于胰腺癌的研究正如火如荼地进行,然而进展仍然不大,尤其是胰腺腺癌的诱发原因迄今不明[119][120][121]。科学家正致力于厘清胰腺腺癌的致病机转,例如KRAS和p53等基因在该疾病中所扮演的角色[45][122][123]。另一项最关键的研究重点之一是病程的进展,特别是糖尿病患者[124],以及癌细胞转移的机制和时间点[125]。
有关胰腺癌的早期诊断仍有正在进行的研究[67][68]。例如,欧洲遗传性胰腺炎和家族性胰腺腺癌(EUROPAC)试验就试图厘清常规筛检是否适用于有胰腺癌家族史和遗传性胰腺腺癌的人[126]。目前已有证据显示新发糖尿病(new onset diabetes)可能为胰腺癌的征兆,这一发现,或许能改善现有的诊断和筛检方法,进而加以预防[124][127]。
另一项研究重点是评估腹腔镜手术的效果是否能超越胰十二指肠切除术,特别是复元时间的差异评估[128]。不可逆性电穿孔(电烧手术)是目前相对常用的烧蚀手术。在病灶尚未扩散的前提下,可有效缩小肿瘤及延长患者存活时间。此类手术适用于生长于胰主要血管以外的肿瘤,以避免造成血管相关的伤害[129][130]。然而单独进行手术的效果不佳,因此通常会同时配合化疗及放射化疗,此种疗法称为辅助治疗(Adjuvant Therapy)。有关辅助疗法的预后仍有争论[2]。后来的试验又于上述的辅助疗法之外,给予其他药物,目前已知最有效的药物为FOLFIRINOX[131]。
新药物的研发也在持续进行中[45][132]。有些试图针对癌细胞的分子途径进行靶向治疗[133][134][135],或降低癌干细胞的抗性[80][136],还有研究尝试改变肿瘤以外的基质及微环境,以降低癌细胞的增殖和转移活性[135][136][137][138][139]。更前瞻的研究还使用了免疫疗法,如溶瘤病毒[140][141]。
去世名人
编辑参见
编辑注释
编辑参考文献
编辑- ^ 1.0 1.1 1.2 1.3 1.4 1.5 1.6 Pancreatic Cancer Treatment (PDQ®) Patient Version. National Cancer Institute. National Institutes of Health. 2014-04-17 [2014-06-08]. (原始内容存档于2014-07-05).
- ^ 2.00 2.01 2.02 2.03 2.04 2.05 2.06 2.07 2.08 2.09 2.10 2.11 2.12 2.13 2.14 2.15 2.16 2.17 2.18 2.19 2.20 2.21 2.22 2.23 2.24 2.25 2.26 2.27 2.28 2.29 Ryan, David P.; Hong, Theodore S.; Bardeesy, Nabeel. Pancreatic Adenocarcinoma. New England Journal of Medicine. 2014-09-11, 371 (11): 1039–1049 [2021-03-16]. ISSN 0028-4793. PMID 25207767. doi:10.1056/NEJMra1404198. (原始内容存档于2021-04-28) (英语).
- ^ 3.00 3.01 3.02 3.03 3.04 3.05 3.06 3.07 3.08 3.09 3.10 3.11 3.12 3.13 3.14 3.15 3.16 3.17 3.18 3.19 3.20 3.21 3.22 3.23 3.24 3.25 3.26 3.27 3.28 Wolfgang, Christopher L.; Herman, Joseph M.; Laheru, Daniel A.; Klein, Alison P.; Erdek, Michael A.; Fishman, Elliot K.; Hruban, Ralph H. Recent progress in pancreatic cancer: Pancreatic Cancer. CA: A Cancer Journal for Clinicians. 2013-09, 63 (5): 318–348. PMC 3769458
 . PMID 23856911. doi:10.3322/caac.21190 (英语).
. PMID 23856911. doi:10.3322/caac.21190 (英语).
- ^ 4.00 4.01 4.02 4.03 4.04 4.05 4.06 4.07 4.08 4.09 Vincent, Audrey; Herman, Joseph; Schulick, Rich; Hruban, Ralph H; Goggins, Michael. Pancreatic cancer. The Lancet. 2011-08, 378 (9791): 607–620 [2021-04-29]. PMC 3062508 . PMID 21620466. doi:10.1016/S0140-6736(10)62307-0. (原始内容存档于2020-10-07) (英语).
- ^ 5.0 5.1 Can pancreatic cancer be prevented?. American Cancer Society. 2014-06-11 [2014-11-13]. (原始内容存档于2014-11-13).
- ^ 6.00 6.01 6.02 6.03 6.04 6.05 6.06 6.07 6.08 6.09 6.10 6.11 6.12 6.13 6.14 World Cancer Report 2014. World Health Organization. 2014. Chapter 5.7. ISBN 92-832-0429-8.
- ^ 7.0 7.1 Cancer Facts & Figures 2010 (PDF). American Cancer Society. 2010 [2014-12-05]. (原始内容 (PDF)存档于2015-01-14). See p. 4 for incidence estimates, and p. 19 for survival percentages.
- ^ Vos, Theo; Allen, Christine; Arora, Megha; Barber, Ryan M; Bhutta, Zulfiqar A; Brown, Alexandria; Carter, Austin; Casey, Daniel C; Charlson, Fiona J. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. The Lancet. 2016-10, 388 (10053): 1545–1602 [2021-04-29]. PMC 5055577 . PMID 27733282. doi:10.1016/S0140-6736(16)31678-6. (原始内容存档于2021-01-24) (英语).
- ^ 9.0 9.1 Wang, Haidong; Naghavi, Mohsen; Allen, Christine; Barber, Ryan M; Bhutta, Zulfiqar A; Carter, Austin; Casey, Daniel C; Charlson, Fiona J; Chen, Alan Zian. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: a systematic analysis for the Global Burden of Disease Study 2015. The Lancet. 2016-10, 388 (10053): 1459–1544 [2021-04-29]. PMC 5388903 . PMID 27733281. doi:10.1016/S0140-6736(16)31012-1. (原始内容存档于2021-02-04) (英语).
- ^ What is Cancer? Defining Cancer. National Cancer Institute, National Institutes of Health. 2014-03-07 [2014-12-05]. (原始内容存档于2014-06-25).
- ^ 11.00 11.01 11.02 11.03 11.04 11.05 11.06 11.07 11.08 11.09 11.10 11.11 11.12 11.13 11.14 11.15 11.16 11.17 11.18 11.19 11.20 11.21 11.22 Bond-Smith, G.; Banga, N.; Hammond, T. M.; Imber, C. J. Pancreatic adenocarcinoma. BMJ. 2012-05-16, 344 (may16 1): e2476–e2476. ISSN 1756-1833. PMID 22592847. doi:10.1136/bmj.e2476 (英语).
- ^ Bussom, Scott; Saif, Muhammad Wasif. Methods and rationale for the early detection of pancreatic cancer. Highlights from the "2010 ASCO Gastrointestinal Cancers Symposium". Orlando, FL, USA. January 22-24, 2010. JOP: Journal of the pancreas. 2010-03-05, 11 (2): 128–130 [2021-03-16]. ISSN 1590-8577. PMID 20208319. (原始内容存档于2021-04-30).
- ^ Shahrokni, Armin; Saif, Muhammad Wasif. Metastatic Pancreatic Cancer: The Dilemma of Quality vs. Quantity of Life. JOP. Journal of the Pancreas. 2013-07-10, Vol 14: 391–394 Paginazione [2021-03-16]. PMID 23846935. doi:10.6092/1590-8577/1663. (原始内容存档于2021-04-24) (英语).
- ^ Bardou, Marc; Le Ray, Isabelle. Treatment of pancreatic cancer: A narrative review of cost-effectiveness studies. Best Practice & Research. Clinical Gastroenterology. 2013-12, 27 (6): 881–892 [2021-01-24]. ISSN 1532-1916. PMID 24182608. doi:10.1016/j.bpg.2013.09.006. (原始内容存档于2021-04-24).
- ^ Pancreatic Cancer Research Fund, 2015. [2017-06-28]. (原始内容存档于2019-02-26).
- ^ Hariharan, D.; Saied, A.; Kocher, H.M. Analysis of mortality rates for pancreatic cancer across the world. HPB. 2008-02, 10 (1): 58–62 [2021-03-16]. PMC 2504856 . PMID 18695761. doi:10.1080/13651820701883148. (原始内容存档于2021-04-24) (英语).
- ^ Lifetime Risk of Developing or Dying From Cancer. American Cancer Society. 2014-10-01 [2014-12-01]. (原始内容存档于2016-11-25).前三名因性别不同而排名不同,包含女性的乳癌,及男性的摄护腺癌。
- ^ 18.0 18.1 Pancreatic Cancer Treatment (PDQ®) Health Professional Version. National Cancer Institute. National Institutes of Health. 2014-02-21 [2014-11-24]. (原始内容存档于2014-10-22). "The highest cure rate occurs if the tumor is truly localized to the pancreas; however, this stage of disease accounts for less than 20% of cases. In cases with localized disease and small cancers (<2 cm) with no lymph node metastases and no extension beyond the capsule of the pancreas, complete surgical resection is associated with an actuarial five-year survival rate of 18% to 24%."
- ^ Harris, Randall E. Epidemiology of Chronic Disease: Global Perspectives. Jones & Bartlett Publishers. 2013: 181–190 [2017-06-21]. ISBN 978-0-7637-8047-0. (原始内容存档于2022-10-13) (英语).
- ^ 20.0 20.1 20.2 20.3 20.4 20.5 20.6 Öberg, K.; Knigge, U.; Kwekkeboom, D.; Perren, A.; ESMO Guidelines Working Group. Neuroendocrine gastro-entero-pancreatic tumors: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Annals of Oncology: Official Journal of the European Society for Medical Oncology. 2012-10,. 23 Suppl 7: vii124–130 [2021-03-16]. ISSN 1569-8041. PMID 22997445. doi:10.1093/annonc/mds295. (原始内容存档于2021-04-24).
- ^ 胡建昆,周总光,杨开清. 胰腺的应用解剖. 世界华人消化杂志. 2001, 9 (7): 826-829 [2021-03-16]. (原始内容存档于2021-04-24).
- ^ Cancer Council NSW. 胰腺癌. Cancer Australia. [2017年2月12日]. (原始内容存档于2021年4月12日).
- ^ 美国癌症协会American Cancer Society & WebMD. 胰腺癌 深藏不露的危機. 亚美医师协会. [2017年2月12日]. (原始内容存档于2017年8月2日).
- ^ 石宜铭,章明珠. 希望之路:面對胰臟癌. 台北: 财团法人癌症希望基金会. 2015.
- ^ 卫生署卫生防护中心 监测及流行病学处. 非傳染病直擊:動起來減低患癌風險 (PDF). 卫生署卫生防护中心 监测及流行病学处. [2017年2月12日]. (原始内容存档 (PDF)于2021年4月24日).
- ^ 新加坡癌症登记处. 癌症统计数据 (PDF). 新加坡癌症登记处. 2013年 [2017年2月12日]. (原始内容 (PDF)存档于2021年4月24日).
- ^ Bussom, Scott; Saif, Muhammad Wasif. Methods and rationale for the early detection of pancreatic cancer. Highlights from the "2010 ASCO Gastrointestinal Cancers Symposium". Orlando, FL, USA. January 22-24, 2010. JOP: Journal of the pancreas. 2010-03-05, 11 (2): 128–130 [2021-04-29]. ISSN 1590-8577. PMID 20208319. (原始内容存档于2021-04-30).
- ^ Govindan R. Chapter 35: Cancer of the Pancreas: Surgical Management. DeVita, Hellman, and Rosenberg's Cancer: Cancer: Principles & Practice of Oncology 9th. Lippincott Williams & Wilkins. 2011. ISBN 978-1-4511-0545-2. Online edition, with updates to 2014
- ^ Neoptolemos, John P.; Abbruzzese, James; Urrutia, Raul A.; Büchler, Markus W. Pancreatic Cancer. Springer Science & Business Media. 2010-01-22: 288 [2017-06-21]. ISBN 978-0-387-77497-8. (原始内容存档于2022-10-19) (英语).
- ^ 30.0 30.1 30.2 Tobias JS, Hochhauser D. Cancer and its Management 7th. 2014: 297. ISBN 978-1-118-46871-5.
- ^ 31.0 31.1 31.2 Types of Pancreas Tumors. The Sol Goldman Pancreas Cancer Research Center. Johns Hopkins Medicine. 2012 [2014-11-18]. (原始内容存档于2014-10-08).
- ^ Farrell, James J.; Fernández-del Castillo, Carlos. Pancreatic Cystic Neoplasms: Management and Unanswered Questions. Gastroenterology. 2013-05, 144 (6): 1303–1315 [2021-03-16]. PMID 23622140. doi:10.1053/j.gastro.2013.01.073. (原始内容存档于2021-04-24) (英语).
- ^ 33.0 33.1 33.2 PanNET在此处采用2010年WHO消化系统疾病分类指引[1] (页面存档备份,存于互联网档案馆)的名称。以往PanNETs曾代表不同的意义,至今仍常用来泛称胰腺内分泌肿瘤。参见:Klimstra, David S.; Modlin, Irvin R.; Coppola, Domenico; Lloyd, Ricardo V.; Suster, Saul. The Pathologic Classification of Neuroendocrine Tumors: A Review of Nomenclature, Grading, and Staging Systems. Pancreas. 2010-08, 39 (6): 707–712. ISSN 0885-3177. doi:10.1097/MPA.0b013e3181ec124e (英语).
- ^ 34.0 34.1 34.2 34.3 34.4 34.5 34.6 34.7 Burns WR, Edil BH. Neuroendocrine pancreatic tumors: guidelines for management and update. Current treatment options in oncology. March 2012, 13 (1): 24–34. PMID 22198808. doi:10.1007/s11864-011-0172-2.
- ^ The Medical Subject Headings indexing system refers to "islet cell carcinoma", which is subdivided into gastrinoma, glucagonoma, somatostatinoma and VIPoma. See: 2014 MeSH tree at "Pancreatic Neoplasms [C04.588.322.475]" 16 October 2014(页面存档备份,存于互联网档案馆)
- ^ 36.0 36.1 Islet Cell Tumors of the Pancreas / Endocrine Neoplasms of the Pancreas. The Sol Goldman Pancreas Cancer Research Center. Johns Hopkins Medicine. 2012 [2015-01-05]. (原始内容存档于2015-01-05).
- ^ 37.0 37.1 37.2 37.3 37.4 37.5 37.6 De La Cruz MS, Young AP, Ruffin MT. Diagnosis and management of pancreatic cancer. Am Fam Physician. April 2014, 89 (8): 626–32. PMID 24784121.
- ^ 38.0 38.1 Alberts, SR; Goldberg, RM. Chapter 9: Gastrointestinal tract cancers. Casciato, DA; Territo, MC (编). Manual of clinical oncology. Lippincott Williams & Wilkins. 2009: 188–236. ISBN 978-0-7817-6884-9.
- ^ Pannala, Rahul; Basu, Ananda; Petersen, Gloria M; Chari, Suresh T. New-onset diabetes: a potential clue to the early diagnosis of pancreatic cancer. The Lancet Oncology. 2009-01, 10 (1): 88–95 [2021-03-17]. PMC 2795483 . PMID 19111249. doi:10.1016/S1470-2045(08)70337-1. (原始内容存档于2021-04-24) (英语).
- ^ Chapter 15; Pancreas. Manual for Staging of Cancer (PDF) 2nd. American Joint Committee on Cancer. : 95–8 [2017-06-21]. (原始内容存档 (PDF)于2014-11-29). See page 95 for citation regarding "... lesser degree of involvement of bones and brain and other anatomical sites."
- ^ Sperti, Cosimo; Moletta, Lucia; Patanè, Giuseppe. Metastatic tumors to the pancreas: The role of surgery. World Journal of Gastrointestinal Oncology. 2014, 6 (10): 381 [2021-04-29]. ISSN 1948-5204. PMC 4197429 . PMID 25320654. doi:10.4251/wjgo.v6.i10.381. (原始内容存档于2021-04-30) (英语).
- ^ Causes of pancreatic cancer. NHS Choices. National Health Service, England. 2014-10-07 [2014-12-05]. (原始内容存档于2014-11-06).
- ^ Bosetti, C.; Lucenteforte, E.; Silverman, D.T.; Petersen, G.; Bracci, P.M.; Ji, B.T.; Negri, E.; Li, D.; Risch, H.A. Cigarette smoking and pancreatic cancer: an analysis from the International Pancreatic Cancer Case-Control Consortium (Panc4). Annals of Oncology. 2012-07, 23 (7): 1880–1888 [2021-04-29]. PMC 3387822 . PMID 22104574. doi:10.1093/annonc/mdr541. (原始内容存档于2020-07-20) (英语).
- ^ Peters, Mary Linton B.; Tseng, Jennifer F.; Miksad, Rebecca A. Genetic Testing in Pancreatic Ductal Adenocarcinoma: Implications for Prevention and Treatment. Clinical Therapeutics. 2016-07, 38 (7): 1622–1635 [2021-04-29]. ISSN 1879-114X. PMID 27041411. doi:10.1016/j.clinthera.2016.03.006. (原始内容存档于2021-04-30).
- ^ 45.0 45.1 45.2 Reznik, Robert; Hendifar, Andrew E.; Tuli, Richard. Genetic determinants and potential therapeutic targets for pancreatic adenocarcinoma. Frontiers in Physiology. 2014, 5 [2021-04-29]. ISSN 1664-042X. PMC 3939680 . PMID 24624093. doi:10.3389/fphys.2014.00087. (原始内容存档于2016-03-05).
- ^ Greenhalf, W.; Grocock, C.; Harcus, M.; Neoptolemos, J. Screening of high-risk families for pancreatic cancer. Pancreatology: official journal of the International Association of Pancreatology (IAP) ... [et al.] 2009, 9 (3): 215–222 [2021-04-29]. ISSN 1424-3911. PMID 19349734. doi:10.1159/000210262. (原始内容存档于2021-04-24).
- ^ Wolfgang, Christopher L.; Herman, Joseph M.; Laheru, Daniel A.; Klein, Alison P.; Erdek, Michael A.; Fishman, Elliot K.; Hruban, Ralph H. Recent progress in pancreatic cancer: Pancreatic Cancer. CA: A Cancer Journal for Clinicians. 2013-09, 63 (5): 318–348. PMC 3769458 . PMID 23856911. doi:10.3322/caac.21190 (英语).
- ^ Pericleous, Marinos; Rossi, Roberta Elisa; Mandair, Dalvinder; Whyand, Tara; Caplin, Martyn Evan. Nutrition and pancreatic cancer. Anticancer Research. 2014-01, 34 (1): 9–21 [2021-03-17]. ISSN 1791-7530. PMID 24403441. (原始内容存档于2021-04-24).
- ^ 49.0 49.1 49.2 Wolfgang CL, Herman JM, Laheru DA, Klein AP, Erdek MA, Fishman EK, Hruban RH. Recent progress in pancreatic cancer. CA: A Cancer Journal for Clinicians. September 2013, 63 (5): 318–48. PMC 3769458 . PMID 23856911. doi:10.3322/caac.21190.
- ^ Lee, Wen-Hwa; Lee, Eva Y.-H. P.; Chen, Yu-Ju; Chen, Yi-Ju; Chang, Yu-Ting; Chang, Ming-Chu; Jeng, Yung-Ming; Hsieh, Ping-Kun; Tien, Sui-Chih. High Glucose Triggers Nucleotide Imbalance through O-GlcNAcylation of Key Enzymes and Induces KRAS Mutation in Pancreatic Cells. Cell Metabolism. 2019-03-07, 0 (0). ISSN 1550-4131. doi:10.1016/j.cmet.2019.02.005.
- ^ Reznik R, Hendifar AE, Tuli R. Genetic determinants and potential therapeutic targets for pancreatic adenocarcinoma. Front Physiol. 2014, 5: 87. PMC 3939680 . PMID 24624093. doi:10.3389/fphys.2014.00087.
- ^ Cancer Facts and Figures 2014 (PDF). American Cancer Society. [2015-01-05]. (原始内容存档 (PDF)于2014-04-29)., p. 19, "Though evidence is still accumulating, consumption of red or processed meat, or meat cooked at very high temperatures, may slightly increase risk."
- ^ Larsson SC, Wolk A. Red and processed meat consumption and risk of pancreatic cancer: meta-analysis of prospective studies. Br J Cancer. January 2012, 106 (3): 603–7 [2017-06-21]. PMC 3273353 . PMID 22240790. doi:10.1038/bjc.2011.585. (原始内容存档于2012-01-15).
- ^ Fitzgerald, J. Edward F.; White, Matthew J.; Lobo, Dileep N. Courvoisier’s Gallbladder: Law or Sign?. World Journal of Surgery. 2009-04-01, 33 (4): 886–891 [2017-07-13]. ISSN 0364-2313. doi:10.1007/s00268-008-9908-y. (原始内容存档于2021-04-24).
- ^ Cyrus Piraka; James M. Scheiman. New Diagnostic Imaging Modalities for Pancreatic Disease. Curr Opin Gastroenterol. 2011, 27 (5) [2017-06-21]. (原始内容存档于2013-11-25).
- ^ 56.0 56.1 56.2 56.3 Seufferlein, T.; Bachet, J. B.; Van Cutsem, E.; Rougier, P.; ESMO Guidelines Working Group. Pancreatic adenocarcinoma: ESMO-ESDO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Annals of Oncology: Official Journal of the European Society for Medical Oncology. 2012-10,. 23 Suppl 7: vii33–40 [2021-03-17]. ISSN 1569-8041. PMID 22997452. doi:10.1093/annonc/mds224. (原始内容存档于2021-04-24).
- ^ Cascinu S, Falconi M, Valentini V, Jelic S. Pancreatic cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Annals of Oncology. May 2010,. 21 Suppl 5: v55–8 [2017-06-21]. PMID 20555103. doi:10.1093/annonc/mdq165. (原始内容存档于2011-08-17).
- ^ 58.0 58.1 58.2 Staging of pancreatic cancer. American Cancer Society. 2014-06-11 [2014-09-29]. (原始内容存档于2020-08-10).
- ^ 59.0 59.1 Zyromski, Nicholas J.; Nakeeb, Attila; Lillemoe, Keith D. Silberman, Howard; Silberman, Allan W. , 编. Principles and practice of surgical oncology : multidisciplinary approach to difficult problems online. Philadelphia: Wolters Kluwer/Lippincott Williams & Wilkins. 2010. Chapter 35 [2014-11-03]. ISBN 978-0-7817-6546-6. (原始内容存档于2015-02-06).
- ^ 60.0 60.1 60.2 60.3 Neuroendocrine tumors, NCCN Guidelines Version 1.2015 (PDF). NCCN Guidelines. National Comprehensive Cancer Network, Inc. 2014-11-11 [2014-12-25]. (原始内容存档 (PDF)于2021-04-24).
- ^ National Cancer Institute. Pancreatic Neuroendocrine Tumors (Islet Cell Tumors) Treatment (PDQ®) Incidence and Mortality [2] (页面存档备份,存于互联网档案馆)
- ^ Delpu Y, Hanoun N, Lulka H, Sicard F, Selves J, Buscail L, Torrisani J, Cordelier P. Genetic and epigenetic alterations in pancreatic carcinogenesis. Curr Genomics. 2011, 12 (1): 15–24. PMC 3129039 . PMID 21886451. doi:10.2174/138920211794520132.
- ^ 63.0 63.1 Lewis MA, Yao JC. Molecular pathology and genetics of gastrointestinal neuroendocrine tumours. Current Opinion in Endocrinology & Diabetes and Obesity. Feb 2014, 21 (1): 22–7. PMID 24310147. doi:10.1097/MED.0000000000000033.
- ^ Thakker RV, Newey PJ, Walls GV, Bilezikian J, Dralle H, Ebeling PR, Melmed S, Sakurai A, Tonelli F, Brandi ML. Clinical practice guidelines for multiple endocrine neoplasia type 1 (MEN1) (PDF). The Journal of Clinical Endocrinology and Metabolism. September 2012, 97 (9): 2990–3011 [2017-06-21]. PMID 22723327. doi:10.1210/jc.2012-1230. (原始内容 (PDF)存档于2015-02-17).
- ^ Diet and activity factors that affect risks for certain cancers: Pancreatic cancer section. American Cancer Society. 2012-08-20 [2014-11-04]. (原始内容存档于2014-11-04).
- ^ Pericleous, Marinos; Rossi, Roberta Elisa; Mandair, Dalvinder; Whyand, Tara; Caplin, Martyn Evan. Nutrition and pancreatic cancer. Anticancer Research. 2014-01, 34 (1): 9–21 [2021-03-17]. ISSN 1791-7530. PMID 24403441. (原始内容存档于2021-04-24).
- ^ 67.0 67.1 He, Xiang-Yi. Advances in pancreatic cancer research: Moving towards early detection. World Journal of Gastroenterology. 2014, 20 (32): 11241 [2021-03-17]. ISSN 1007-9327. PMC 4145762 . PMID 25170208. doi:10.3748/wjg.v20.i32.11241. (原始内容存档于2021-04-24) (英语).
- ^ 68.0 68.1 68.2 Okano, Keiichi. Strategies for early detection of resectable pancreatic cancer. World Journal of Gastroenterology. 2014, 20 (32): 11230 [2021-03-17]. ISSN 1007-9327. PMC 4145761 . PMID 25170207. doi:10.3748/wjg.v20.i32.11230. (原始内容存档于2021-04-24) (英语).
- ^ Stoita, Alina. Review of screening for pancreatic cancer in high risk individuals. World Journal of Gastroenterology. 2011, 17 (19): 2365 [2021-03-17]. ISSN 1007-9327. PMC 3103788 . PMID 21633635. doi:10.3748/wjg.v17.i19.2365. (原始内容存档于2021-04-24) (英语).
- ^ Gurusamy, Kurinchi Selvan; Kumar, Senthil; Davidson, Brian R.; Fusai, Giuseppe. Resection versus other treatments for locally advanced pancreatic cancer. The Cochrane Database of Systematic Reviews. 2014-02-27, (2): CD010244 [2021-03-18]. ISSN 1469-493X. PMID 24578248. doi:10.1002/14651858.CD010244.pub2. (原始内容存档于2021-04-24).
- ^ 71.0 71.1 Mollberg, Nathan; Rahbari, Nuh N.; Koch, Moritz; Hartwig, Werner; Hoeger, Yumiko; Büchler, Markus W.; Weitz, Jürgen. Arterial Resection During Pancreatectomy for Pancreatic Cancer: A Systematic Review and Meta-Analysis. Annals of Surgery. 2011-12, 254 (6): 882–893. ISSN 0003-4932. PMID 22064622. doi:10.1097/SLA.0b013e31823ac299 (英语).
- ^ 72.0 72.1 72.2 Pancreatic adenocarcinoma. NCCN Guidelines Version 1.2015 (PDF). NCCN Guidelines. National Comprehensive Cancer Network, Inc. 2014-12-04 [2014-12-26]. (原始内容存档 (PDF)于2007-02-08).
- ^ Álamo, José M. Improving outcomes in pancreatic cancer: Key points in perioperative management. World Journal of Gastroenterology. 2014, 20 (39): 14237 [2021-03-18]. ISSN 1007-9327. PMC 4202352 . PMID 25339810. doi:10.3748/wjg.v20.i39.14237. (原始内容存档于2021-04-24) (英语).
- ^ Lopez, Nicole E. Borderline resectable pancreatic cancer: Definitions and management. World Journal of Gastroenterology. 2014, 20 (31): 10740 [2021-03-18]. ISSN 1007-9327. PMC 4138454 . PMID 25152577. doi:10.3748/wjg.v20.i31.10740. (原始内容存档于2021-04-24) (英语).
- ^ Polistina, Francesco; Natale, Giuseppe Di; Bonciarelli, Giorgio; Ambrosino, Giovanni; Frego, Mauro. Neoadjuvant strategies for pancreatic cancer. World Journal of Gastroenterology. 2014-07-28, 20 (28): 9374–9383 [2021-03-18]. PMC 4110569 . PMID 25071332. doi:10.3748/wjg.v20.i28.9374. (原始内容存档于2021-04-24) (英语).
- ^ Gillen, Sonja; Schuster, Tibor; Meyer zum Büschenfelde, Christian; Friess, Helmut; Kleeff, Jörg. Seiler, Christoph , 编. Preoperative/Neoadjuvant Therapy in Pancreatic Cancer: A Systematic Review and Meta-analysis of Response and Resection Percentages. PLoS Medicine. 2010-04-20, 7 (4): e1000267. ISSN 1549-1676. PMC 2857873 . PMID 20422030. doi:10.1371/journal.pmed.1000267 (英语).
- ^ Christians, Kathleen K.; Evans, Douglas B. Additional support for neoadjuvant therapy in the management of pancreatic cancer. Annals of Surgical Oncology. 2015-06, 22 (6): 1755–1758 [2021-03-18]. ISSN 1534-4681. PMID 25519932. doi:10.1245/s10434-014-4307-0. (原始内容存档于2021-04-24).
- ^ Tsvetkova, E.V.; Asmis, T.R. Role of Neoadjuvant Therapy in the Management of Pancreatic Cancer: Is the Era of Biomarker-Directed Therapy Here?. Current Oncology. 2014-08-01, 21 (4): 650–657 [2021-03-18]. ISSN 1718-7729. PMC 4117630 . PMID 25089113. doi:10.3747/co.21.2006. (原始内容存档于2021-04-24) (英语).
- ^ Zhan, Han-xiang; Xu, Jian-wei; Wu, Dong; Zhang, Tai-ping; Hu, San-yuan. Pancreatic cancer stem cells: new insight into a stubborn disease. Cancer Letters. 2015-02-28, 357 (2): 429–437 [2021-03-18]. ISSN 1872-7980. PMID 25499079. doi:10.1016/j.canlet.2014.12.004. (原始内容存档于2021-04-24).
- ^ 80.0 80.1 Tanase, Cristiana Pistol. Cancer stem cells: Involvement in pancreatic cancer pathogenesis and perspectives on cancer therapeutics. World Journal of Gastroenterology. 2014, 20 (31): 10790 [2021-03-18]. ISSN 1007-9327. PMC 4138459 . PMID 25152582. doi:10.3748/wjg.v20.i31.10790. (原始内容存档于2021-04-24) (英语).
- ^ Allen, Victoria B; Gurusamy, Kurinchi Selvan; Takwoingi, Yemisi; Kalia, Amun; Davidson, Brian R. Cochrane Upper GI and Pancreatic Diseases Group , 编. Diagnostic accuracy of laparoscopy following computed tomography (CT) scanning for assessing the resectability with curative intent in pancreatic and periampullary cancer. Cochrane Database of Systematic Reviews. 2016-07-06. PMC 6458011 . PMID 27383694. doi:10.1002/14651858.CD009323.pub3 (英语).
- ^ Heinemann, V.; Haas, M.; Boeck, S. Neoadjuvant treatment of borderline resectable and non-resectable pancreatic cancer. Annals of Oncology: Official Journal of the European Society for Medical Oncology. 2013-10, 24 (10): 2484–2492 [2021-03-18]. ISSN 1569-8041. PMID 23852311. doi:10.1093/annonc/mdt239. (原始内容存档于2021-04-24).
- ^ 83.0 83.1 83.2 Thota, Ramya; Pauff, James M.; Berlin, Jordan D. Treatment of metastatic pancreatic adenocarcinoma: a review. Oncology (Williston Park, N.Y.). 2014-01, 28 (1): 70–74 [2021-03-18]. ISSN 0890-9091. PMID 24683721. (原始内容存档于2021-04-24).
- ^ Ryan, DP. Chemotherapy for advanced exocrine pancreatic cancer: Topic 2475, Version 46.0 (subscription required). UpToDate. Wolters Kluwer Health. 2014-07-08 [2014-11-18]. (原始内容存档于2014-12-08).
- ^ Cancer Drug Information: FDA Approval for Erlotinib Hydrochloride. National Cancer Institute. National Institutes of Health. 2013-07-03 [2014-12-05]. (原始内容存档于2014-11-29).
- ^ Borazanci, Erkut; Von Hoff, Daniel D. Nab-paclitaxel and gemcitabine for the treatment of patients with metastatic pancreatic cancer. Expert Review of Gastroenterology & Hepatology. 2014-09, 8 (7): 739–747 [2021-03-18]. ISSN 1747-4132. PMID 24882381. doi:10.1586/17474124.2014.925799. (原始内容存档于2021-04-24).
- ^ Falconi M, Bartsch DK, Eriksson B, Klöppel G, Lopes JM, O'Connor JM, Salazar R, Taal BG, Vullierme MP, O'Toole D. ENETS Consensus Guidelines for the management of patients with digestive neuroendocrine neoplasms of the digestive system: Well-differentiated pancreatic non-functioning tumors. Neuroendocrinology. 2012, 95 (2): 120–34. PMID 22261872. doi:10.1159/000335587.
- ^ Jensen RT, Cadiot G, Brandi ML, de Herder WW, Kaltsas G, Komminoth P, Scoazec JY, Salazar R, Sauvanet A, Kianmanesh R. ENETS Consensus Guidelines for the management of patients with digestive neuroendocrine neoplasms: Functional pancreatic endocrine tumor syndromes. Neuroendocrinology. 2012, 95 (2): 98–119. PMC 3701449 . PMID 22261919. doi:10.1159/000335591.
- ^ Pavel M, Baudin E, Couvelard A, Krenning E, Öberg K, Steinmüller T, Anlauf M, Wiedenmann B, Salazar R. ENETS Consensus Guidelines for the management of patients with liver and other distant metastases from neuroendocrine neoplasms of foregut, midgut, hindgut, and unknown primary. Neuroendocrinology. 2012, 95 (2): 157–76. PMID 22262022. doi:10.1159/000335597.
- ^ Rossi, Roberta Elisa; Massironi, Sara; Conte, Dario; Peracchi, Maddalena. Therapy for metastatic pancreatic neuroendocrine tumors. Annals of Translational Medicine. 2014-01, 2 (1) [2017-07-14]. ISSN 2305-5839. PMC 4200651 . PMID 25332984. doi:10.3978/j.issn.2305-5839.2013.03.01. (原始内容存档于2021-04-24).
- ^ Nick Mulcahy. FDA Approves Lanreotide for Neuroendocrine Tumors. Medscape Medical News. WebMD LLC. 2014-12-17 [2014-12-25]. (原始内容存档于2015-01-18).
- ^ Everolimus Approved for Pancreatic Neuroendocrine Tumors (页面存档备份,存于互联网档案馆) The ASCO Post. May 15, 2011, Volume 2, Issue 8
- ^ National Cancer Institute. Cancer Drug Information. FDA Approval for Sunitinib Malate (页面存档备份,存于互联网档案馆). Pancreatic Neuroendocrine Tumors
- ^ Tejani, Mohamedtaki Abdulaziz; Saif, Muhammad Wasif. Pancreatic neuroendocrine tumors: does chemotherapy work?. JOP: Journal of the pancreas. 2014-03-10, 15 (2): 132–134 [2017-07-14]. ISSN 1590-8577. PMID 24618436. (原始内容存档于2020-05-10).
- ^ Text is available electronically (but may require free registration) See: Benson AB, Myerson RJ, Sasson AR. Pancreatic, neuroendocrine GI, and adrenal cancers. Cancer Management: A Multidisciplinary Approach 13th edition 2010.. [2017-06-21]. ISBN 978-0-615-41824-7. (原始内容存档于2011-05-15).
- ^ Gulenchyn KY, Yao X, Asa SL, Singh S, Law C. Radionuclide therapy in neuroendocrine tumours: A systematic review. Clinical Oncology. 2012, 24 (4): 294–308. PMID 22221516. doi:10.1016/j.clon.2011.12.003.
- ^ Vinik AI. Advances in Diagnosis and Treatment of Pancreatic Neuroendocrine Tumors (PNETS). Endocrine Practice. 2014, 20 (11): 1–23. PMID 25297671. doi:10.4158/EP14373.RA.
- ^ Kwekkeboom DJ, de Herder WW, van Eijck CH, Kam BL, van Essen M, Teunissen JJ, Krenning EP. Peptide receptor radionuclide therapy in patients with gastroenteropancreatic neuroendocrine tumors. Seminars in Nuclear Medicine. 2010, 40 (2): 78–88. PMID 20113677. doi:10.1053/j.semnuclmed.2009.10.004.
- ^ Bodei L, Cremonesi M, Kidd M, Grana CM, Severi S, Modlin IM, Paganelli G. Peptide receptor radionuclide therapy for advanced neuroendocrine tumors. Thoracic Surgery Clinics. 2014, 24 (3): 333–49. PMID 25065935. doi:10.1016/j.thorsurg.2014.04.005.
- ^ Castellano D, Grande E, Valle J, Capdevila J, Reidy-Lagunes D, O'Connor JM, Raymond E. Expert consensus for the management of advanced or metastatic pancreatic neuroendocrine and carcinoid tumors. Cancer Chemotherapy and Pharmacology. 2014, 75 (6): 1099–114. PMID 25480314. doi:10.1007/s00280-014-2642-2.
- ^ Singh S, Dey C, Kennecke H, Kocha W, Maroun J, Metrakos P, Mukhtar T, Pasieka J, Rayson D, Rowsell C, Sideris L, Wong R, Law C. Consensus Recommendations for the Diagnosis and Management of Pancreatic Neuroendocrine Tumors: Guidelines from a Canadian National Expert Group. Annals of Surgical Oncology. 2014, 22 (8): 2685–99. PMID 25366583. doi:10.1245/s10434-014-4145-0.
- ^ Palliative or Supportive Care. American Cancer Society. 2014 [2014-08-20]. (原始内容存档于2014-08-21).
- ^ Buanes TA. Pancreatic cancer-improved care achievable. World Journal of Gastroenterology. 2014-08-14, 20 (30): 10405–18. PMC 4130847 . PMID 25132756. doi:10.3748/wjg.v20.i30.10405.
- ^ If treatment for pancreatic cancer stops working. American Cancer Society. 2014-06-11 [2014-08-20]. (原始内容存档于2014-10-22).
- ^ Arcidiacono PG, Calori G, Carrara S, McNicol ED, Testoni PA. Arcidiacono PG , 编. Celiac plexus block for pancreatic cancer pain in adults. Cochrane Database Syst Rev. 2011, (3): CD007519. PMID 21412903. doi:10.1002/14651858.CD007519.pub2.
- ^ J. S. Barkin, R. I. Goldberg, G. N. Sfakianakis & J. Levi. Pancreatic carcinoma is associated with delayed gastric emptying. Digestive diseases and sciences. 1986, 31 (3): 265–267. PMID 3004847.
- ^ Cancer Facts and Figures 2014 (PDF). American Cancer Society. [2015-01-05]. (原始内容存档 (PDF)于2014-04-29)., Table, p. 18, rates adjusted for normal life expectancy
- ^ Lozano, Rafael; Naghavi, Mohsen; Foreman, Kyle; Lim, Stephen; Shibuya, Kenji; Aboyans, Victor; Abraham, Jerry; Adair, Timothy; Aggarwal, Rakesh. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. The Lancet. 2012-12-15, 380 (9859): 2095–2128 [2021-03-17]. ISSN 0140-6736. PMID 23245604. doi:10.1016/S0140-6736(12)61728-0. (原始内容存档于2016-05-06) (英语).
- ^ Siegel, Rebecca L.; Miller, Kimberly D.; Jemal, Ahmedin. Cancer statistics, 2016. CA: a cancer journal for clinicians. 2016-01-01, 66 (1): 7–30 [2017-06-21]. ISSN 1542-4863. PMID 26742998. doi:10.3322/caac.21332. (原始内容存档于2020-05-13).
- ^ What are the key statistics about pancreatic cancer?. American Cancer Society. 2014-06-11 [2014-11-11]. (原始内容存档于2014-11-11).
- ^ Pancreatic cancer statistics. Cancer Research UK. [2014-12-18]. (原始内容存档于2014-12-18).; "In 2010, in the UK, the lifetime risk of developing pancreatic cancer is 1 in 73 for men and 1 in 74 for women", noting "The lifetime risk ... has been calculated ... using the 'Current Probability' method; this is a different method used from most other cancer sites since the possibility of having more than one diagnosis of pancreatic cancer over the course of their lifetime is very low"
- ^ Pancreatic cancer statistics. Cancer Research UK. [2014-10-28]. (原始内容存档于2014-10-06).
- ^ 113.0 113.1 Pancreatic cancer: yesterday, today and tomorrow. Future Oncology. 2016-06-01, 12 (16): 1929–1946 [2017-07-13]. ISSN 1479-6694. doi:10.2217/fon-2016-0010. (原始内容存档于2022-04-20).
- ^ 114.0 114.1 114.2 Busnardo, A. C.; DiDio, L. J.; Tidrick, R. T.; Thomford, N. R. History of the pancreas. American Journal of Surgery. 1983-11, 146 (5): 539–550 [2021-03-17]. ISSN 0002-9610. PMID 6356946. doi:10.1016/0002-9610(83)90286-6. (原始内容存档于2021-04-24).
- ^ 115.0 115.1 115.2 115.3 Are, Chandrakanth; Dhir, Mashaal; Ravipati, Lavanya. History of pancreaticoduodenectomy: early misconceptions, initial milestones and the pioneers. HPB. 2011-06, 13 (6): 377–384 [2021-03-17]. PMC 3103093 . PMID 21609369. doi:10.1111/j.1477-2574.2011.00305.x. (原始内容存档于2021-04-24) (英语).
- ^ 116.0 116.1 Cameron, John L.; Riall, Taylor S.; Coleman, JoAnn; Belcher, Kenneth A. One Thousand Consecutive Pancreaticoduodenectomies:. Annals of Surgery. 2006-07, 244 (1): 10–15. ISSN 0003-4932. PMC 1570590 . PMID 16794383. doi:10.1097/01.sla.0000217673.04165.ea (英语).
- ^ Govindan R. DeVita, Hellman, and Rosenberg's Cancer: Cancer: Principles & Practice of Oncology 9th. Lippincott Williams & Wilkins. 2011. Chapter 35: Cancer of the Pancreas: Surgical Management. ISBN 978-1-4511-0545-2. Online edition, with updates to 2014
- ^ Fernández-del Castillo, Carlos; Morales-Oyarvide, Vicente; McGrath, Deborah; Wargo, Jennifer A.; Ferrone, Cristina R.; Thayer, Sarah P.; Lillemoe, Keith D.; Warshaw, Andrew L. Evolution of the Whipple procedure at the Massachusetts General Hospital. Surgery. 2012-09, 152 (3): S56–S63 [2021-03-17]. PMC 3806095 . PMID 22770961. doi:10.1016/j.surg.2012.05.022. (原始内容存档于2021-04-24) (英语).
- ^ Wolpin, Brian M.; Stampfer, Meir J. Defining determinants of pancreatic cancer risk: are we making progress?. Journal of the National Cancer Institute. 2009-07-15, 101 (14): 972–973 [2021-03-17]. ISSN 1460-2105. PMID 19561317. doi:10.1093/jnci/djp182. (原始内容存档于2021-04-24).
- ^ What's new in pancreatic cancer research and treatment?. American Cancer Society. 2014-06-11 [2014-07-17]. (原始内容存档于2016-11-29).
- ^ Pancreatic cancer research. Cancer Research UK. [2014-07-17]. (原始内容存档于2014-02-18).
- ^ Australian Pancreatic Genome Initiative. Garvan Institute. [2014-07-17]. (原始内容存档于2014-07-26).
- ^ Australian Pancreatic Cancer Genome Initiative; Biankin, Andrew V.; Waddell, Nicola; Kassahn, Karin S.; Gingras, Marie-Claude; Muthuswamy, Lakshmi B.; Johns, Amber L.; Miller, David K.; Wilson, Peter J. Pancreatic cancer genomes reveal aberrations in axon guidance pathway genes. Nature. 2012-11, 491 (7424): 399–405 [2021-03-17]. ISSN 0028-0836. PMC 3530898 . PMID 23103869. doi:10.1038/nature11547. (原始内容存档于2021-04-24) (英语).
- ^ 124.0 124.1 Pannala, Rahul; Basu, Ananda; Petersen, Gloria M; Chari, Suresh T. New-onset diabetes: a potential clue to the early diagnosis of pancreatic cancer. The Lancet Oncology. 2009-01, 10 (1): 88–95 [2021-03-17]. PMC 2795483 . PMID 19111249. doi:10.1016/S1470-2045(08)70337-1. (原始内容存档于2021-04-24) (英语).
- ^ Graham, J. S.; Jamieson, N. B.; Rulach, R.; Grimmond, S. M.; Chang, D. K.; Biankin, A. V. Pancreatic cancer genomics: where can the science take us?. Clinical Genetics. 2015-09, 88 (3): 213–219 [2021-03-17]. ISSN 1399-0004. PMID 25388820. doi:10.1111/cge.12536. (原始内容存档于2021-04-25).
- ^ About EUROPAC. European Registry of Hereditary Pancreatitis and Familial Pancreatic Cancer (EUROPAC). University of Liverpool. [2014-07-17]. (原始内容存档于2014-07-26).
- ^ Bruenderman, Elizabeth H.; Martin, Robert C.G. High-risk population in sporadic pancreatic adenocarcinoma: guidelines for screening. Journal of Surgical Research. 2015-03, 194 (1): 212–219 [2021-03-17]. PMC 4559279 . PMID 25479908. doi:10.1016/j.jss.2014.06.046. (原始内容存档于2021-04-24) (英语).
- ^ Subar, D.; Gobardhan, P.D.; Gayet, B. Laparoscopic pancreatic surgery. Best Practice & Research Clinical Gastroenterology. 2014-02, 28 (1): 123–132 [2021-03-17]. doi:10.1016/j.bpg.2013.11.011. (原始内容存档于2021-04-24) (英语).
- ^ Weiss, Matthew J.; Wolfgang, Christopher L. Irreversible electroporation: a novel pancreatic cancer therapy. Current Problems in Cancer. 2013-09, 37 (5): 262–265 [2021-03-17]. ISSN 1535-6345. PMID 24331180. doi:10.1016/j.currproblcancer.2013.10.002. (原始内容存档于2021-04-24).
- ^ Moir, J.; White, S. A.; French, J. J.; Littler, P.; Manas, D. M. Systematic review of irreversible electroporation in the treatment of advanced pancreatic cancer. European Journal of Surgical Oncology: The Journal of the European Society of Surgical Oncology and the British Association of Surgical Oncology. 2014-12, 40 (12): 1598–1604 [2021-03-17]. ISSN 1532-2157. PMID 25307210. doi:10.1016/j.ejso.2014.08.480. (原始内容存档于2021-04-24).
- ^ Hackert, Thilo; Sachsenmaier, Milena; Hinz, Ulf; Schneider, Lutz; Michalski, Christoph W.; Springfeld, Christoph; Strobel, Oliver; Jäger, Dirk; Ulrich, Alexis. Locally Advanced Pancreatic Cancer. Annals of Surgery: 457–463. doi:10.1097/sla.0000000000001850.
- ^ Al Haddad, Amal H. I.; Adrian, Thomas E. Challenges and future directions in therapeutics for pancreatic ductal adenocarcinoma. Expert Opinion on Investigational Drugs. 2014-11, 23 (11): 1499–1515 [2021-03-17]. ISSN 1744-7658. PMID 25078674. doi:10.1517/13543784.2014.933206. (原始内容存档于2021-04-24).
- ^ Adiseshaiah, Pavan P.; Crist, Rachael M.; Hook, Sara S.; McNeil, Scott E. Nanomedicine strategies to overcome the pathophysiological barriers of pancreatic cancer. Nature Reviews Clinical Oncology. 2016-12, 13 (12): 750–765 [2021-03-17]. ISSN 1759-4774. doi:10.1038/nrclinonc.2016.119. (原始内容存档于2021-04-24) (英语).
- ^ Kleger, A.; Perkhofer, L.; Seufferlein, T. Smarter drugs emerging in pancreatic cancer therapy. Annals of Oncology: Official Journal of the European Society for Medical Oncology. 2014-07, 25 (7): 1260–1270 [2021-03-17]. ISSN 1569-8041. PMID 24631947. doi:10.1093/annonc/mdu013. (原始内容存档于2021-04-24).
- ^ 135.0 135.1 Tang, Shing-Chun. Novel therapeutic targets for pancreatic cancer. World Journal of Gastroenterology. 2014, 20 (31): 10825 [2017-06-21]. ISSN 1007-9327. PMC 4138462 . PMID 25152585. doi:10.3748/wjg.v20.i31.10825. (原始内容存档于2014-12-29) (英语).
- ^ 136.0 136.1 Schober, Marvin; Jesenofsky, Ralf; Faissner, Ralf; Weidenauer, Cornelius; Hagmann, Wolfgang; Michl, Patrick; Heuchel, Rainer; Haas, Stephan; Löhr, J.-Matthias. Desmoplasia and Chemoresistance in Pancreatic Cancer. Cancers. 2014-10-21, 6 (4): 2137–2154 [2021-03-17]. ISSN 2072-6694. PMC 4276960 . PMID 25337831. doi:10.3390/cancers6042137. (原始内容存档于2021-04-24) (英语).
- ^ Rossi, Maria L. Therapeutic options for the management of pancreatic cancer. World Journal of Gastroenterology. 2014, 20 (32): 11142 [2021-03-17]. ISSN 1007-9327. PMC 4145755 . PMID 25170201. doi:10.3748/wjg.v20.i32.11142. (原始内容存档于2021-04-24) (英语).
- ^ Neesse, Albrecht; Krug, Sebastian; Gress, Thomas M.; Tuveson, David A.; Michl, Patrick. Emerging concepts in pancreatic cancer medicine: targeting the tumor stroma. OncoTargets and Therapy. 2013-12-18, 7: 33–43 [2021-03-17]. ISSN 1178-6930. PMC 3872146 . PMID 24379681. doi:10.2147/OTT.S38111. (原始内容存档于2021-04-24).
- ^ Heinemann, V.; Reni, M.; Ychou, M.; Richel, D. J.; Macarulla, T.; Ducreux, M. Tumour-stroma interactions in pancreatic ductal adenocarcinoma: rationale and current evidence for new therapeutic strategies. Cancer Treatment Reviews. 2014-02, 40 (1): 118–128 [2021-03-17]. ISSN 1532-1967. PMID 23849556. doi:10.1016/j.ctrv.2013.04.004. (原始内容存档于2021-04-24).
- ^ Fong, Yuman; Ady, Justin; Heffner, Jacqueline; Klein, Elizabeth. Oncolytic viral therapy for pancreatic cancer: current research and future directions. Oncolytic Virotherapy. 2014-02: 35 [2021-03-17]. ISSN 2253-1572. PMC 4918362 . PMID 27512661. doi:10.2147/OV.S53858. (原始内容存档于2018-06-02) (英语).
- ^ Pavelic, Jasminka. Editorial: combined cancer therapy. Current Pharmaceutical Design. 2014, 20 (42): 6511–6512 [2021-03-17]. ISSN 1873-4286. PMID 25341927. doi:10.2174/1381612820666140826154834. (原始内容存档于2021-04-24).
外部链接
编辑